There is no set of labs or set of symptoms that can answer this question. This question can be answered by reflection of your experience, current symptoms, and concerns paired with evaluation from a healthcare provider versed in peri/menopause. (You can go to The Menopause Society or The International Society For The Study of Women’s Sexual Health to find one near you!)
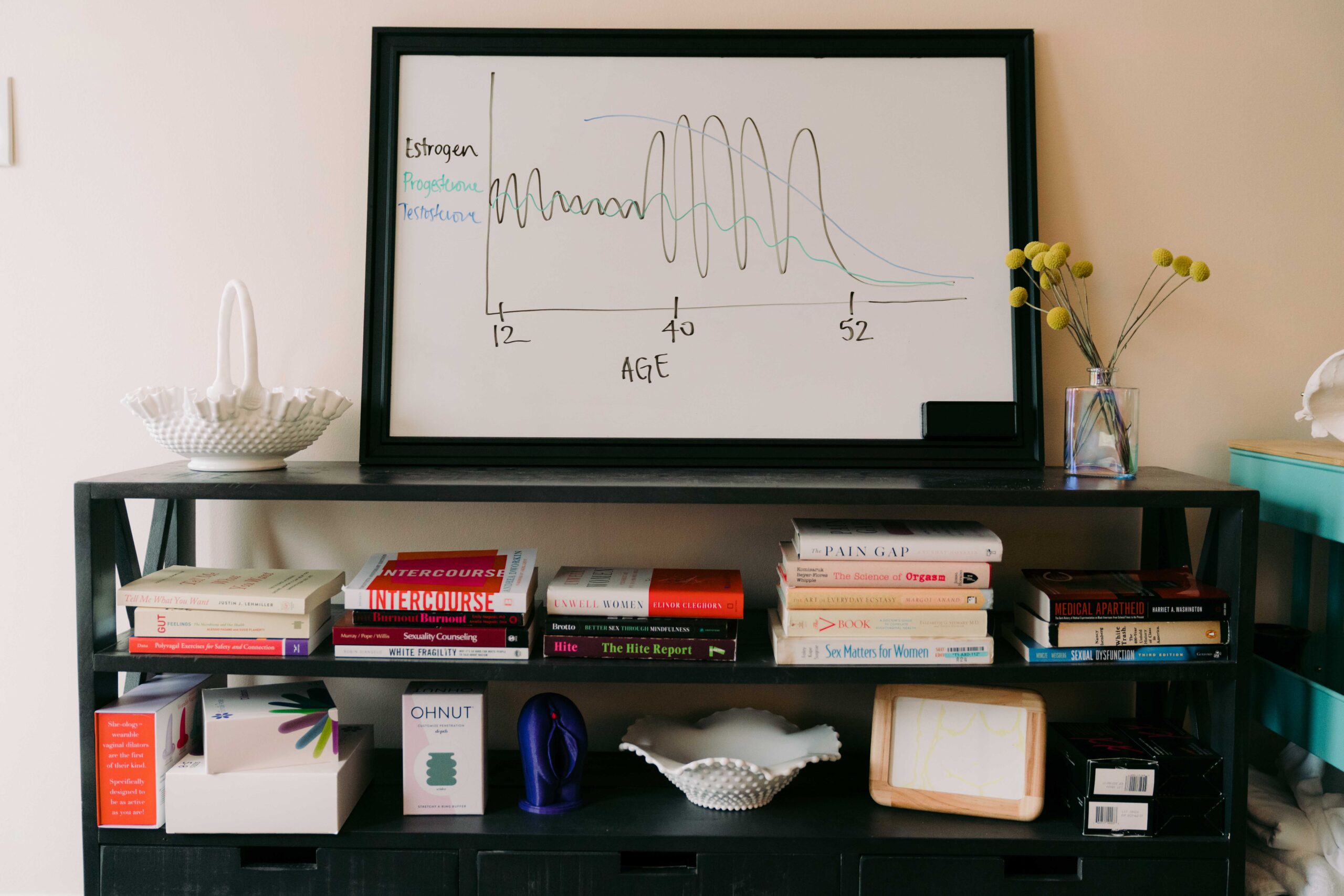
Simply put, perimenopause is puberty but backwards. It’s a time of great hormonal fluctuation, which leads to physical, emotional, and sexual symptoms. There are many symptoms of perimenopause! I can’t even list them all out here, and I learn about new ones almost every week as I work with patients. The most common are listed below:
• Mood changes such as irritability, new or worsening anxiety, insomnia either trouble falling asleep or staying asleep, depression, mood swings, rage.
• Brain fog, trouble concentrating, trouble with word finding.
• Decrease in libido or difficulty with orgasm.
• Night sweats, hot flashes, or trouble regulating your body temperature.
• Irregular periods – periods too close together, periods too far apart, bleeding that lasts longer, more clots or more cramping.
• Joint pain.
• Fatigue.
• Skin changes including dry skin, itchy skin, rashes, hair loss on your head but hair growth in unwanted places like on your face, oily skin and acne.
• Genitourinary changes including vaginal dryness, pain with sex, urinary urgency or frequency, incontinence, recurrent UTIs, sensations feeling like a UTI but your last UTI test came back “normal”.
Okay, that’s a lot and I am sure I missed some (such as ringing in the ear!). It’s complex, and everyone’s experience is unique. You may also feel like you aren’t experiencing ANY OF THIS, and that is okay too!
Hormonal options
Geez, there’s a lot out there. To see all the options that I currently use, you can view this free guide to menopausal hormone therapy. Hint – this requires an individualized approach! You could also consider birth control pills, as they contain synthetic estrogens and progestins or progestin only.
Whether you choose menopausal hormone therapy or birth control pills, hormone therapy is not a one size fits all and you must remain open and curious to change things up.
Here are 4 factors to consider when you are thinking about whether to start (or continue) hormonal birth control or start peri/menopausal hormone therapy:
1. Do you need contraception? If you do not want to have a pregnancy AND your partner is a cis-gendered male who has not had a vasectomy, then this is something to consider! If you are still menstruating, pregnancy is possible especially during perimenopause. Menopausal hormone therapy is not birth control.
2. Do you have contraindications to birth control? Some people who have high blood pressure or who have previous blood clots or clotting disorder may fall into a category in which oral birth control pills are contraindicated. However, someone with high blood pressure, history of blood clots, or clotting disorder may be a candidate for certain types of peri/menopausal hormone therapy. Not all hormones are created equal!
3. Did you have side effects when you were on birth control? Some women have side effects such as mood disturbances, pelvic pain, decreased libido. The reason for that is the route in which you take birth control (orally) and/or the types of hormones that are in birth control (hello synthetic estrogens and progestins). If that’s the case, you may be a candidate for per/menopausal hormone therapy because these are different types of hormones (body-identical) and we can use different routes (ie transdermal).
4. Do you have breakthrough symptoms on birth control? Occasionally some women will still have breakthrough perimenopausal symptoms on birth control pills, and if that is the case they should have a conversation about menopausal hormone therapy (with a plan for contraception in place if that is necessary).
But, it’s not only symptoms that we are trying to address. There is also a preventative aspect for menopausal hormone therapy. Do you have a family history of osteoporosis? Do you have a personal history of prediabetes? Do you have a family history of colon cancer, or you yourself at high risk for colon cancer? Menopausal hormone therapy has been shown to prevent osteoporosis (actually has an FDA indication for this), diabetes and colon cancer. In certain situations, it also may prevent cardiovascular disease.
Perimenopause management is not all about hormone therapy. It is important to take a comprehensive approach and consider sleep hygiene, exercise strategies, nutrition intake, micronutrient support, mental health, and stress reduction.




{kind=link}
{kind=link}
{kind=link}
{kind=link}